
The Vaccine Question - The Next #59
A deep dive into a controversial topic
Hi there, and welcome to The Next - my take on health, wellness, and company building.
In the last few years I’ve founded 3 health brands (Kettle & Fire, Perfect Keto, Surely non-alc wine). I’m now working on Truemed, which allows health and wellness brands to accept HSA/FSA funds. Previously, I worked in tech and had no experience in CPG, DTC, or any other 3-letter industries.
If you missed past episodes, I recommend checking out The Great American Poisoning, my manifesto on what’s going on with our chronic disease crisis. Otherwise, let’s dive in!
The vaccine question
I’ll be honest: I’m nervous to send this. But the debate around vaccines today is so unbearably stupid and low-resolution that I wanted to spend time digging into the topic.
So, let’s talk vaccines.
The vaccine conversation today is so polarized. Every conversation goes one of two ways:
Vaccines are always good, there are zero risks for anyone taking them ever. Anyone who says otherwise is an anti-science Luddite!
Vaccines are always evil, Bill Gates is trying to microchip everyone, and they are solely responsible for autism, obesity, inflation, and every Bad Health Thing of the past decades!
This conversation is dumb.
What if I give my kid every vaccine but one: does that make me an anti-vaxxer?
What if I think the 2017, 54-shot schedule is the right one, not the 73-shot schedule the CDC currently recommends?
What if I think the Swiss vaccine schedule is better (fewer shots, more spaced out). Does that make me an anti-vaxxer? Or what if I have my reservations about the 2025 schedule that recommends 99 shots (and 2 COVID vaccines)?
Today’s vaccine conversation has no room for nuance. I’d like that to change.
Part 1: The Incentive Landscape
First, let’s start with some facts.
In 1962, children received 5 vaccine doses. Today, the recommended vaccine schedule is 72 doses of 16 different vaccine formulations. Next year, the CDC recommends that babies more than 6 months old receive 2 COVID vaccines before turning 4.
Obviously, the schedule has hugely increased, most notably after 1986. Why?
In 1986, many lawsuits were filed against vaccine makers for their DPT vaccine causing brain damage and sudden infant death. In a reaction to the lawsuit, makers of the DPT vaccine threatened to cease making vaccines if they continued to be exposed to legal liability for producing them.
The result of this threat was the passage of the 1986 National Childhood Vaccine Injury Act, a law that removed a vaccine maker’s liability for any injuries caused by their products. In effect, vaccine makers would no longer be financially liable for injuries or deaths caused by their vaccines (unlike drug manufacturers who do retain liability).
Since this act was passed, the vaccine schedule has exploded. If you are 41 or older, you have had fewer vaccines in your lifetime than the average 6-month-old today.

Now, I understand why this was considered a good idea! Suppose you believed that DPT and other vaccines were miracle drugs that severely injured or killed some small portion of the population (and - because these are childhood vaccination schedules - almost entirely children). In that case, I understand how a cost-benefit analysis could point towards vaccinating everyone. If your options are truly “nobody gets vaccinated, everyone gets DPT” or “everyone gets vaccinated, some small percentage of the population is adversely impacted”, I understand how this act could make sense!
Whatever the rationale, the passage of the 1986 act led to an explosion of new vaccines, and the vaccine schedule grew 5x in just 37 years.
Imagine you’re Pfizer, and you now have a suite of products that are (1) very profitable, (2) come with no downside or liability risk, and (3) are effectively mandated by the CDC. What do you think - do you make more or less of these kinds of products? The answer, empirically, has been more.
This is a dream business: a profitable product, sold without liability (and covered by insurance) to a customer base that is effectively mandated to take it by the CDC.
The National Childhood Vaccine Injury Act wasn’t passed without any guardrails. In exchange for this blanket liability protection, the Department of Health and Human Services promised to conduct safety reviews every two years and report them to Congress.
Unfortunately, it appears they haven’t followed through on that obligation. After being sued to produce these records in 2018, HHS admitted they had never conducted any of the required safety testing and never issued a report to Congress as required by law.
Lack of safety reviews with the blanket liability shield is not a good combination of incentives. Yet as I dug in, that’s not the only skewed incentive around all things vaccines. You see, the CDC also owns 57 vaccine patents, and spent $4.9 of its $12.0 billion-dollar annual budget buying and distributing vaccines!
Additionally, as part of a royalty program, government employees and regulators involved with the creation and licensure of vaccine patents also receive royalties, which in many cases can comprise a significant part of their overall income.
Again, if you squint, you can see how this policy makes sense. The CDC, NIH, and other government organizations spend billions of dollars doing basic research. If and when industry turns that research into products they profit from, why shouldn’t they receive some portion of the upside?
It’s also easy to see how these royalty payments could create an incentive for scientists and regulators to approve more and more vaccines. These incentives can be quite large: 2400 scientists from the NIH received $325M+ in royalty payments between 2009 and 2020!
It’s not just the regulators: doctors are financially incentivized to push vaccines as well. In the 2016 Blue Cross, Blue Shield provider incentive program, Blue Cross Blue Shield paid a $40,000 bonus to fully vaccinate 100 patients. Anthem has similar incentives in place, and pay doctors bonuses for each vaccinated member. That bonus goes up as more members are vaccinated:
Again - I can understand why this might make sense! If you think vaccines are a public health miracle, if insurance companies want to incentivize doctors to push (what they view as) the world’s safest and most effective intervention on all of their patients… this could make sense!
Unfortunately, many doctors and states go far beyond recommending vaccines to patients. In some states like California, you’re effectively not allowed to opt your child out of the vaccination schedule, even for religious or medical exemptions. California even passed a law that contains harsh penalties for granting exemptions and has a process to review any doctor who writes more than 5 over their career.
To my knowledge, vaccines are unique among health interventions in terms of how they’re mandated. Given how bad the incentive landscape is around all things vaccines, I think it’s worth taking a hard look at whether or not this web of incentives leads to their overuse and over-scheduling.
Part 2: the impact of vaccines on health
Every health intervention has risks and rewards. Eat a carrot, run the risk of choking (or get carotenemia, where your skin turns orange lol). Get invasive surgery to cure appendicitis, run the risk of infection (and death). Many of our most common healthcare interventions (chemo, drugs, etc) all come with some kind of risk, as well as potential upside.
Vaccines are no different. Their purpose is to forever alter one’s immune system after just 1-2 injections. That’s powerful, and comes with the same risks and rewards as any intervention. That’s why, when I hear people say that questioning vaccine safety is somehow “anti-science”, I get confused. Is it anti-science to question another drug's side effects? Of course not.
In fact, we know that some vaccines, at least some of the time, cause injury. Reports of vaccine injuries — any negative health outcome caused by a vaccine — and vaccine-related deaths are made in the Vaccine Adverse Event Reporting System (VAERS), a passive surveillance system run jointly by the FDA and the CDC. Most reports are made by nurses, doctors, and other medical professionals, and submitting a fraudulent report is a felony. Tens of thousands of vaccine injuries are reported every year, even though few people are aware of VAERS (and submitting reports is time-consuming).

It’d be surprising if vaccines were the only medical intervention humanity has discovered that was completely safe, completely effective, and had zero side effects. Judging by the fact that prior vaccines have been withdrawn from the market (this is one list I’ve found) due to safety concerns, we certainly cannot say these interventions are always 100% safe and effective. Could the risk/reward of every vaccine be worthwhile? Absolutely! But to say they have no side effects or downsides is just wrong.
There are also concerns about how vaccines are determined safe (or not).
The gold standard pharmaceutical trial is a double-blinded randomized, controlled trial using an inert placebo. Unfortunately, no vaccine on the childhood schedule has completed such a trial. Typically, vaccines are tested against older vaccines. Those vaccines in turn were tested against even older vaccines, or they were never subjected to a controlled trial at all:

Obviously, the most that a trial of this kind can determine is whether or not a new vaccine is as safe as an older one. And given the fact that controlled trials are mostly not conducted, the definitive scientific evidence to say that these compounds “do not cause” specific diseases does not exist.
Not only are these vaccines only tested against other vaccines (and not a null control group), but vaccine makers are also not required to test for interactions with other vaccines, or test for potential problems associated with combined, simultaneous injections of multiple vaccines! Negative effects of drug interactions are shockingly common and can occur in up to 45% of the time a patient is given multiple prescription medications. Why would this not be looked at with vaccines?
Given that the vaccine schedule has hugely increased since 1986, we should absolutely be running studies to ensure that vaccines administered in combination are safe. This whole issue reminds me of how we regulate (or don’t) many of the chemicals in our food system: we never test for interactions between chemical compounds.
There is a fair bit of research pointing to vaccines administered in combination may come with increased risk. For example, this study on Florida’s Medicaid database found there was a significant increase in adverse events associated with vaccines, and that the number of these diseases went up as more vaccines were administered.

A similar study compared health outcomes between vaccinated and unvaccinated children, and found that vaccinated children had increased rates of asthma, infection, and gastrointestinal disorders.
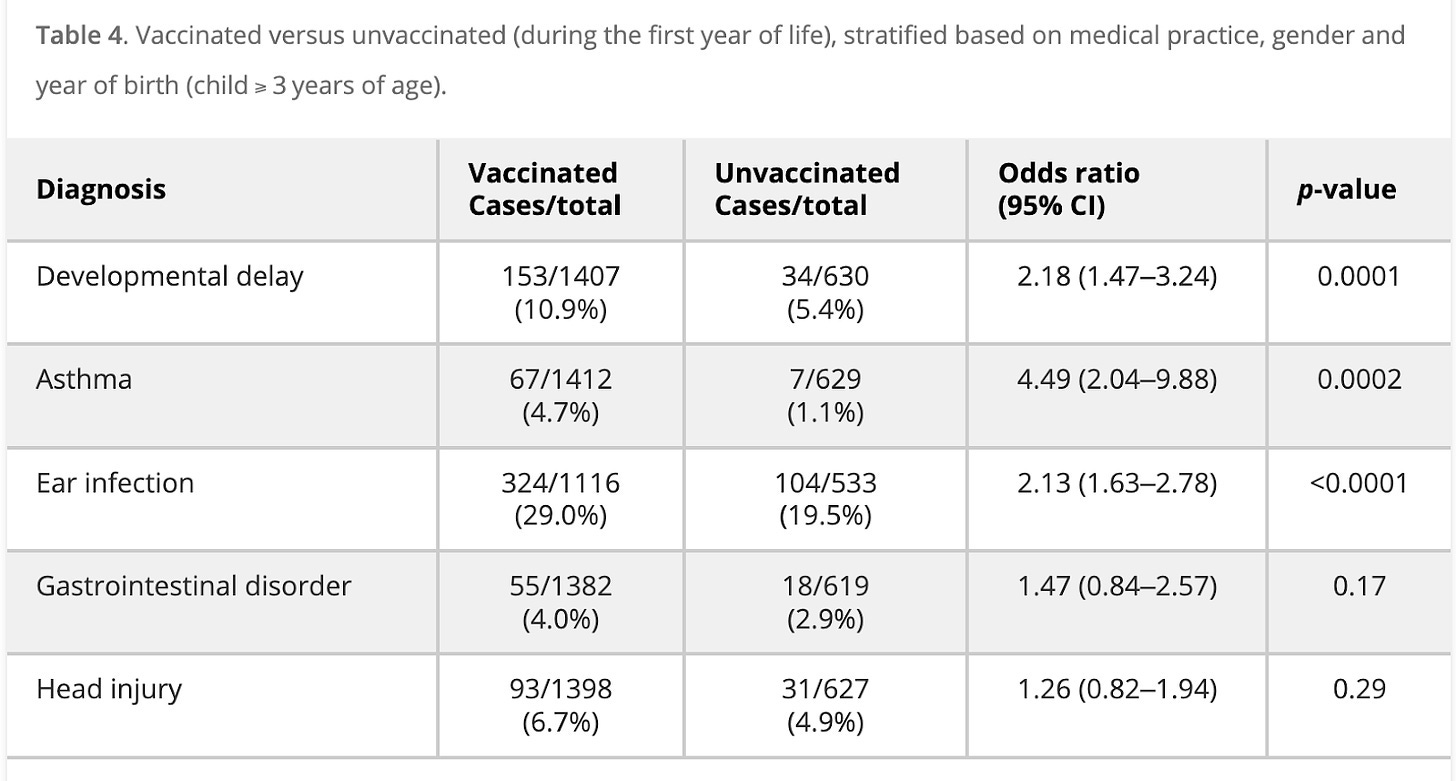
Hooker BS, Miller NZ. Analysis of health outcomes in vaccinated and unvaccinated children: Developmental delays, asthma, ear infections and gastrointestinal disorders. SAGE Open Medicine. 2020;8. doi:10.1177/2050312120925344
And a recent (citizen science) survey of 10,000 parents showed an association of vaccine shots with ADHD and autism diagnosis. The more shots given, the likelier a diagnosis of a developmental disorder:

Other studies have shown a similar dose-dependent relationship between the number of vaccines administered and an increase in various chronic conditions (see this excellent overview for more). As Brad summarizes in that post:
There have been other studies that have compared vaccinated versus unvaccinated children and the incidence of chronic diseases. Here is a list of seven such studies I was able to find. I summarized the findings across them for a few select diseases in a chart.

The results are clear and have a high degree of corroboration across studies. Vaccinated children are much sicker than unvaccinated children. They have a higher incidence of chronic diseases like allergies, ADHD, asthma, autism, and frequent infections. Each of these findings has been replicated in at least three independent studies. Certain studies also found vaccinated children were more commonly inflicted with Eczema, Learning Disabilities, Neurodevelopmental Disorders, Pneumonia, Ear Infections, GI Disorders, Asthma, Developmental Delays, Fevers, Pink Eye, Breathing Issues, Eating Disorders, Respiratory Infections, Behavioral Issues, Anemia, Throat inflammation, Convulsions, Infections, Seizure, Hospitalization, Sleep Issues, and Speech Disorders (see collected data here).
In short, I think it’s quite possible that even if every vaccine is safe and effective, the combination and frequency of today’s vaccine schedule could be responsible for many potential health concerns.
Part 3: why might vaccines be harmful?
In the days of old, patients were infected with live pathogens to create a strong immune response. For the patient, this sucked: you would be exposed to a small amount of a pathogen, get sick, and hope you recovered (and were thus inoculated). Many died from smallpox and other pathogens of the day during attempted vaccinations.
Vaccines today pair a protein with a toxin meant to induce a strong immune response. It’s similar to how scientists induce peanut allergies in lab animals, by stimulating an animal’s immune system with a toxin while feeding them peanuts. The animal’s immune system associates the toxin with the peanuts and will generate a strong immune response to peanut exposure in the future.
Many vaccines operate under the same principle: stimulate the immune system with a toxin so that the immune system responds the next time it encounters that compound. These ingredients are called “adjuvants”, and are designed to create a strong response in the immune system. Here are some adjuvants often used in vaccines:
Aluminum (implicated in brain damage and neurodegenerative diseases)
Formaldehyde (carcinogenic, banned in Europe)
Beta-Propiolactone (carcinogenic)
GMO Yeast, Bacterial and Viral DNA, Dairy/Egg Components (can cause allergies)
Glutaraldehyde (can cause birth defects in animals)
Peanut & Soybean Oil (can create allergies)
Animal and Human Cells (foreign substances can cause rejection, leukemia, diabetes)
Mercury (highly toxic)
MSG (linked to birth defects, developmental delays, infertility, banned in Europe)
Neomycin Sulphate (interferes with B6 absorption)
Phenol/Phenoxyethanol (antifreeze, toxic)
Polysorbate 80 & 20 (carcinogenic)
Here is a list of adjuvants in several common vaccines:
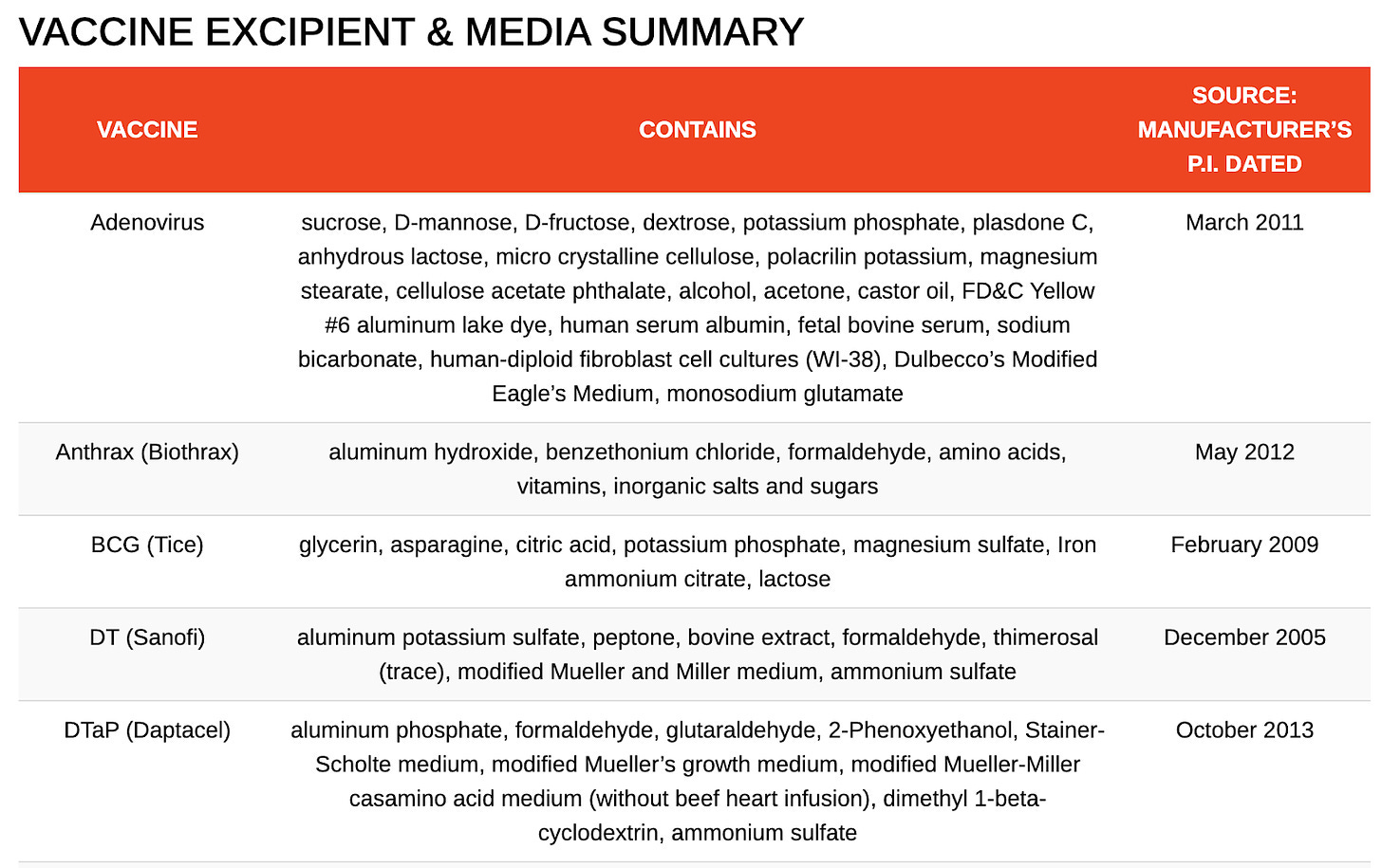
These compounds are certainly not good when consumed, and are quite likely worse when simply injected (as the body has no way to clear some of these toxic compounds like it does through digestion).
Unfortunately, this can be a big deal. Aluminum (for example) is more efficiently absorbed when injected into the body versus when eaten. When ingested, the body efficiently filters out aluminum in the GI tract and prevents its absorption, allowing only 0.1%-0.3% into the body. Vaccines given in the first six months of life (per the CDC schedule) contain 3,675 mcg of aluminum.
Aluminum serves no function in the body. It is neurotoxic, neurodegenerative, toxic to bone tissue, and may contribute to autoimmune disorders. In the 1990s, there were reports of babies dying and becoming developmentally impaired after receiving IVs contaminated with aluminum, which led to the FDA setting a limit on daily aluminum exposure.
According to the FDA, they should be limited to 4-5 mcg/kg/day, though even these levels can cause toxicity. That is equivalent to a limit of 20 mcg for an 8lb baby, or 50 mcg for a 20lb baby. There is no aluminum-containing vaccine on the schedule which is below this limit.

Given the ample evidence of aluminum’s toxicity, I was quite surprised to dig in and see just how much aluminum a baby would be exposed to by following the current CDC schedule.
I’d like to pause here and simply say that safety and efficacy are important. If vaccines do not, in fact, cause harm, we should be able to research and ask that question! Just a few years after lies about COVID origins (and many questions around vaccine safety), digging further into the science around vaccine safety should be applauded by all sides.
With no RCTs on safety (either in a vacuum or in combination), one is left to your own devices to understand the risks and rewards associated with each vaccine. This seems silly: let’s run the experiments, publish the data freely, and move past our current equilibrium where we both mandate these for everyone and do next to no testing on their health impacts. Clear and transparent research would go a long way to progress today’s polarized debate.
Part 4: vaccine risks and rewards
As I said at the beginning of this piece: just because vaccines as a category of health intervention have risks, does not mean that they’re not worth doing! This is the crux of the vaccine discussion we should be having: what are the specific risk/reward tradeoffs for each vaccine on today’s schedule? How should we think about them?
For more on this topic, Brad does an exceptional job of writing about the risk/reward tradeoff for each vaccine here, as does another anonymous doctor here. I’d encourage reading each one.
As we said, these are serious interventions! But if you look closely, I firmly believe the current schedule has some questionable vaccines. For example, the Hepatitis B vaccine.
The Hepatitis B vaccine is recommended for children at birth, even though practically the only way to get it is via sexual activity or a blood transfusion (and the mother is tested before giving birth). There have been 137,676 adverse events associated with the Hepatitis B vaccine reported to VAERS, including 2,337 deaths. Additionally, neither Switzerland nor Austria recommend the vaccine for low-risk babies at birth.
When I see things like this on the schedule, it seems to me like just a bad risk/reward tradeoff. It seems absurd to give an infant a vaccine that you can only get from STDs or blood transfusions… and - even if you get it - the immunity expires after ~10 years!
Additionally, the new recommendation for children between 6 months and 4 years old to get the COVID vaccine seems far more profit-motivated than rooted in good science. According to the WHO, children under 5 represent less than 0.1% of global COVID deaths (about 1,902 deaths). Many studies find adverse reactions to mRNA at a rate of 0.125%, and we know that these vaccines are not exactly effective, and (in the case of young children) are preventing nearly zero deaths. Why add them to the schedule?
It’s this part that frustrates me. I look around at American children in the throes of a chronic disease crisis. Their lunches are filled with crap, they’re offered soda at every turn, and nearly 30% of kids have diabetes or prediabetes.
Against this landscape, we aren’t mandating healthy meals, we aren’t banning processed foods from cafeterias, we aren’t forcing kids to get outside and exercise. Yet when it comes to vaccinating a 6-month-old against a disease that will almost certainly not kill them, where immunity wears off within a year, and where they are more likely to have an adverse reaction than they are to die from COVID, we mandate that intervention? Come on.
Where does this leave me?
The conversation on vaccines needs to evolve. The simple “anti-vaxxer vs vax” spectrum makes no sense in a complicated world where the number, type, and combinatorial effects of vaccines have changed so much over the previous decades.
What if I agree with today’s schedule, but have reservations about the CDC’s new recommendation to give mRNA vaccines to all children: does that make me an anti-vaxxer? What if I prefer the Swiss vaccine schedule, or the vaccine schedule that US parents used in 1986?
I strongly believe each person can and should make their own cost-benefit decision when it comes to vaccines. That said, for me the data points to shifting the vaccine schedule.
In my view, it’s kind of insane to expose an infant to multiple doses of these powerful interventions in such a short period of time. Today’s vaccine schedule was created for convenience, and doctors recommend so many shots so soon after birth primarily because they are concerned that parents won’t return for future shots!
I think it’s safe to say that a child following the 1986 schedule is probably safer than one following today’s schedule. I also think that it’s quite a good thing that polio, mumps, and other diseases have been eradicated.
Where that leaves me personally: is fewer shots, more spaced out, (and a hell of a lot more research please). This approach is effectively the same as the one advocated for by Paul Thomas, author of The Vaccine-Friendly Plan, whose approach to spacing resulted in a dramatically lower rate of vaccine injuries. It’s also similar to the schedule followed by many countries in the EU: fewer shots, more spaced out.
Today’s epidemics are not acute diseases like mumps, polio, and the like. Rather, they’re chronic conditions: food allergies, obesity, inflammation, and others like ADHD and autism. Given the incentive landscape surrounding these interventions, I strongly believe that taking a second look at the existing schedule (and clamoring for more research) is required.
😌 Dope stuff on the internet
Some of my favorite things since the last newsletter (note: I don’t get paid to recommend anything here):
📰 Article - I really enjoyed this post on how to turn ideas into progress. I’m very hopeful that we are on the precipice of a much-needed return to a lighter regulatory regime, and entering a time where all kinds of technology and other progress will accelerate.
📚 Book rec - I’ve been on a kick to read more about the founding fathers and the history of the American Revolution. As governance is top of mind, I’ve really enjoyed reading 1776, John Adam’s biography, and the Federalist Papers. Governance is a hard problem, and reading history has given me an appreciation for just how hard it was, and the tradeoffs made and debated by the founding fathers.
⌚ Cool product - A friend recently sent me the (all glass, no plastic) new Aeropress, and it’s great! It’s been a great upgrade to my morning coffee routine, and makes great coffee. Which I often then ruin (according to coffee purists) by adding peanut butter collagen to it.
Also, if you’re looking to stay on top of your health and get your labs done, Superpower is a good option. Skip the waitlist using my link!
🎵 Music - This mix is exceptional, made by one of my friends just getting into the DJ game! I have a few friends who are getting more serious about music mixing and production, and it’s made me interested in exploring it further at some point in the distant future when I have more time 😂.
🏀 Random - A friend recently mentioned my hair is getting a little thin on top. So I’m going to try a bunch of interventions for 90 days (and write about it after!) to see what changes. After reading about the many serious downsides of finasteride, definitely planning to stay away from that stuff.
🔥Hot take - SSRIs are much, much worse than commonly suspected. Numerous large studies show half of those prescribed SSRIs quit using them because they cannot tolerate their side effects, over half of users develop sexual dysfunction, half of SSRI users experience significant withdrawals when they stop the drugs. Additionally a variety of other side effects also exist (e.g., users frequently report becoming emotionally anesthetized to life and taking an SSRI during pregnancy significantly increases the risk of a fetal birth defect).
Given that something like 25% of women are on SSRIs today, it seems kinda important to discuss the tradeoffs that exist with these widely prescribed set of drugs?🙋♂️ Ask - The team at Perfect Keto is conducting a citizen science trial for people who want to improve their heart markers without going on statins. If that’s you, fill out this form: you’ll get discounted labs and free product in exchange for sharing your lab data pre and post-intervention.
***
I’d love your thoughts on the above. I’m nervous to send this, as conversations around vaccines are so fraught with emotions. That said, I think it’s an important conversation to have, and my hope is that I can slightly move the Overton window in a direction that allows for a more rational conversation around one of the most intense medical interventions we subject ourselves to.
Justin
In my physician experience, actually a lot of people have a nuanced view on vaccines; picking and choosing which to take (or their own schedules for boosting etc) - it's just the online discourse and politics of it all that are polarized, (as is true of most online discourse and politics these days).
A few things jump out from my knowledge base here as overly skewed against vaccines.
1) If you look at correlational data of course of course it looks like sicker people get more vaccines. They legitimately are higher risk individuals that may be making the rational choice to vaccinate more often (eg. my parents made me get the flu shot growing up only because I had asthma). Additionally, they are interfacing with the healthcare system more often, generally, and so have both more opportunity and more rapport with healthcare workers to take what is recommended. Moreover, the people who are healthcare-seeking are going to get quite a lot more "diagnoses" than those that never visit the doctor, even if the disease burden is the same. There is a reason RCTs are the gold standard...
2) For Hep B specifically, of course, there is a reason this became the protocol (doctors are not just torturing babies for no reason: if it makes no sense look harder). Vaccination at birth prevents vertical transmission from mom to baby which was a very common mode of transmission, and one that results in particularly high levels of chronic infection (as opposed to the immune system beating the infection). Testing mom is not fool proof as there are window periods where infection gets missed. And despite waning antibody titers - which do not reflect the full scope of immune memory - childhood vaccination seems to give good long term protection not just for 10 years. The rates of hep B have fallen dramatically thanks to this vaccine - and even still, deaths from hep B still remain higher than *correlated* reports of death in the time period after vaccination which largely are not thought to be causative.
I agree with you, and regularly preach that everything we do in medicine, as in life, has risks and benefits. We should of course continuously scrutinize those risks and benefits both in our public health recommendations and in our individual decision making. Can we make them without as much gross ingredients? Should the incentives be changed? I don't have insider knowledge on those fronts. But vaccinations are overall a huge benefit of modern medicine and something we do that is actually preventative in a broken sick care system so let's not lose sight of that.
THANK YOU FOR THIS!! Finally, someone put into words what I try to explain. I don’t consider myself antivax but the ridiculous number that my doc tries to talk me into—every time I have an appointment—is annoying. I try to take care of my immune system through healthy choices and stress reduction. If I decide not to take a vaccine, that should be my gamble.
This article in clear detail show the massive changes to the vaccine schedule since I was a child (1960s). But I I ever question it, I’m told I don’t believe in science. Belief is the very antithesis of science!!!